Chest wall deformity is an important category of disease in thoracic surgery, mainly referring to abnormalities in chest wall appearance and structure. Regardless of the cause, these deformities can alter chest wall structure and may affect both physical health and psychological well-being. Clearly distinguishing between primary and secondary chest wall deformities is crucial for accurate diagnosis, treatment selection, and surgical planning.
Basic Concepts and Classification of Chest Wall Deformity
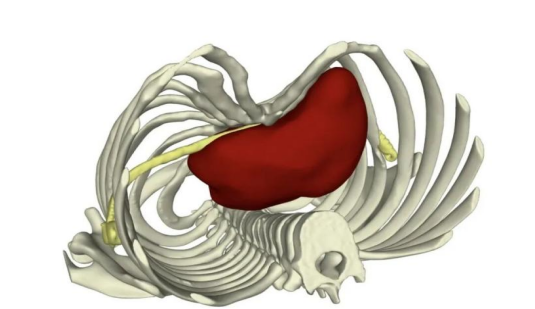
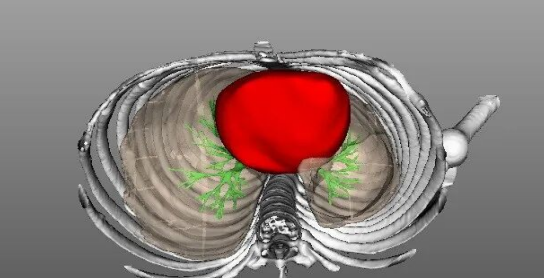
The chest wall consists of three main components: skin, soft tissue, and bony structures.
- Soft tissue: Primarily includes superficial breast tissue, muscle, fat, and intercostal structures
- Bony structures: Primarily includes the sternum, costal cartilage, and ribs
Chest wall deformity mainly refers to the abnormality of the bony structures of the chest wall.
Chest wall deformity covers a wide range. Clinically, common chest wall deformities include pectus excavatum, pectus carinatum, barrel chest, flat chest, and asphyxiating thoracic dystrophy (Jeune syndrome), among others.
However, chest wall deformity can be divided into two major categories based on etiology: primary chest wall deformity and secondary chest wall deformity.
Learn more about specific chest wall deformity types:
6 Common Types of Chest Wall Deformities
5 Commonly Misdiagnosed Chest Wall Deformities
Primary Chest Wall Deformity
Primary chest wall deformity refers to a condition with unknown etiology or a condition whose pathological lesions originate from the organ or system itself, not directly caused by other known diseases or external factors.
The exact cause of primary chest wall deformity remains unknown, but it is most often present at birth and is considered a congenital condition. Many current studies suggest that primary chest wall deformity is related to genetic factors, gene mutations, and embryonic developmental abnormalities.
Some examples:
- In chest wall surgical diseases, chest wall deformities are mostly related to genetic factors, such as pectus excavatum, pectus carinatum, and flat chest. Many patients have a family history, with multiple family members exhibiting the same condition, indicating a clear genetic predisposition.
- Familial asphyxiating thoracic dystrophy (ATD), also known as Jeune syndrome, is a rare autosomal recessive genetic disorder.
Secondary Chest Wall Deformity
The biggest difference between secondary and primary chest wall deformity is the presence of a clear etiology. The causative factors of secondary chest wall deformity can come from multiple sources. Clinically, there are three common causes: trauma, surgery, and disease.
Trauma-Induced Chest Wall Deformity
Trauma is the most common cause of secondary chest wall deformity, usually resulting from severe impact or compression. Typical cases involve multiple rib fractures or a sternum fracture. Improper fracture healing alters chest shape, leading to chest wall deformity.
Depending on the early fixation management, three typical outcomes may occur clinically:
- Early non-fixation of fracture: Lack of timely fixation leads to malunion, resulting in late-stage chest wall deformity. Late-stage deformities are severe and complex, significantly increasing surgical costs.
- Early fixation with ideal outcome: Chest wall deformity is prevented.
- Early fixation with poor outcome: This type of deformity is relatively simple to manage at the early stage, and correction can be achieved with proper fixation alone.
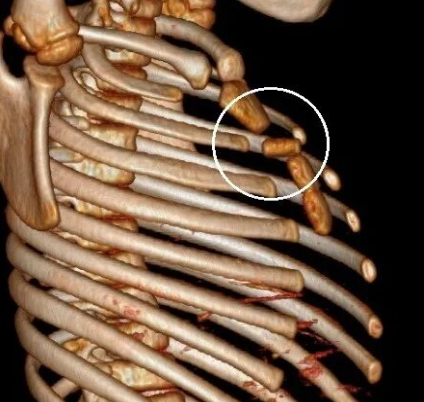
Chest wall deformity caused by sternum fracture
Surgery-Induced Chest Wall Deformity
Surgery-related chest wall deformities are categorized as either expected or unexpected: the former are actively embraced as a necessary cost of treatment, and the latter are undesirable sequelae of surgical failure.
1. Expected Deformity
Such deformities are an unavoidable cost (a side effect) of the surgical procedure. For example:
- Thoracoplasty for chronic empyema: The surgical purpose is to selectively remove partial ribs to cause chest wall collapse and eliminate the pus cavity, thereby treating chronic empyema. Treating the disease is the surgical goal, while deformity is an unavoidable cost. Modern modified procedures (such as the Schede procedure) are more precise, attempting to remove only the necessary ribs to minimize aesthetic deformity and impact on respiratory function.
- Thoracic surgery via rib bed incision: This incision method is commonly used in traditional thoracic surgery, requiring the removal or partial cutting of ribs to enter the thoracic cavity. Although this incision choice was reasonable at that time, improper healing after rib removal often leads to chest wall deformity.
2. Unexpected Deformity
This type of chest wall deformity results from surgery itself or a failure that causes an unexpected deformity.
- Cardiac surgery commonly leads to complications such as pectus excavatum.
- Bar displacement or tilting after conventional Nuss surgery may result in new asymmetric chest wall deformities requiring reoperation.
Moreover, it is worth noting that prior surgery causes adhesions within the chest cavity, significantly increasing the difficulty and risk of secondary surgery.
Chest wall deformity after failed Nuss procedure
Disease-Induced Chest Wall Deformity
Disease-induced deformities are also common. Diseases alter the chest through chronic traction, compression, or compensation. For example, lateral chest wall collapse caused by chronic empyema, barrel chest caused by chronic respiratory diseases (such as emphysema), and flat chest caused by chronic wasting diseases or lung diseases.
Additionally, there are some easily overlooked chest wall deformities secondary to other chest wall conditions. Such as those secondary to chest wall tumor resection defects, large chest wall defect repairs, or severe chest wall infection fibrosis. Due to the primary disease attracting main attention, these secondary chest wall deformities are often ignored.

Left chronic empyema with pleural thickening and calcification, accompanied by marked asymmetry of the bilateral chest wall
Main Risks of Chest Wall Deformities
Chest wall deformities can affect patients both physiologically and psychologically.
Physiological Risks:
The integrity and stability of the chest wall structure are the foundation for chest wall function. When the chest wall structure is damaged, chest wall function is affected, manifesting various functional abnormalities. Harm varies by deformity type and severity.
Protruding deformities generally do not compress the heart or lungs; the protective function of the chest wall structure for internal organs remains intact. In contrast, depressed deformities, such as severe pectus excavatum, can directly compress the heart and lungs, causing symptoms like palpitations, shortness of breath, and dyspnea. Additionally, in some patients with severe or long-standing pectus excavatum, the anterior chest wall depression compresses the heart and push it toward the left side. After the heart shifts, it pulls the mediastinal structures to the left, leading to uneven force distribution on both sides of the spine, which may result in scoliosis.
Furthermore, secondary chest wall deformities are mostly caused by specific diseases. For example, barrel chest is typically caused by emphysema and usually appears only when the disease progresses to the middle or late stage, serving as an important sign of the underlying disease. In such cases, the respiratory symptoms (caused by the underlying disease) of patients with barrel chest become more severe.
Psychological Risks:
Chest wall deformity alters chest wall appearance, causing psychological impact on patients, damaging self-esteem, triggering emotional distress, and a series of psychological problems. In severe cases, it may even lead to mental illness.
For example, pectus excavatum and pectus carinatum often progress rapidly during adolescence, a critical period for self-esteem development. Adolescents and young people with pectus excavatum and pectus carinatum bear psychosocial burdens, including body image damage, social anxiety, and reduced quality of life, typically manifesting as social avoidance, concealment behavior, and emotional distress (such as low self-esteem, irritability, poor concentration).
ICWS's Chest Wall Deformity Treatment
Treatment of chest wall deformities focuses on restoring function and appearance. ICWS has over 15 years of research and clinical experience in chest wall conditions, being the world's first independent chest wall disorder surgical treatment institution and also the world's largest chest wall deformity correction center.
Patients or families considering treatment or correction of chest wall deformities are encouraged to contact ICWS for consultation and evaluation.