Flat pectus carinatum is a rare chest wall deformity that, while resembling pectus carinatum in appearance, significantly differs in bone structure. Therefore, the surgical treatments effective for pectus carinatum are not applicable to this condition. To ensure a precise diagnosis and appropriate treatment, Dr. Wenlin Wang has named this condition flat pectus carinatum, distinctly differentiating it from pectus carinatum.
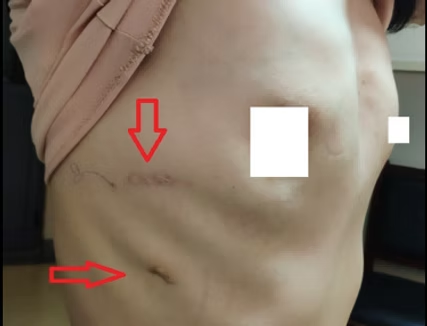
Essentially, flat pectus carinatum is one of the complex chest wall deformities characterized by both concavity and convexity. It manifests as a forward protrusion of the anterior chest wall, accompanied by a localized vertical groove-like depression in the center.